yourTMJ Guidebook: What is TMJ and How Can You Treat It?

There is no short answer to this question. Anyone who says there is is either uninformed, or trying to trick you.
So if you're the type of person who wants to ACTUALLY understand TMJ; who's done with oversimplified B.S on Google; who's tired of endlessly scrolling forums and support groups... I spent the last year writing this for you.
By the end, you will fundamentally understand what TMJ Disorder is, why it happens and what you can do to start fixing it TODAY. There is no other TMJ literature in existence that does so much to tie everything together for the patient perspective.
So buckle up for a long read - it may be lifechanging.
If you want to download this as a PDF with a table of contents, you can here.

Introduction
Hi, I'm Noam. I’m not a Dentist. I’m not a PT. I’m not a surgeon. But I am an Ivy League educated engineer who - over the past 5 years - has made it my mission to understand TMJ Disorders to their core. I’ve interviewed hundreds of patients, dozens of doctors, and read almost every piece of research I could get my hands on.
The sad thing for me is that, knowing what I know now, I could’ve prevented what may now be irreversible TMJ damage. My goal is to pass it on to you.
The important thing is that there is a LOT of noise in the TMJ space. And there’s a lot of bias. Which is why I wanted to write this document - to share patient to patient the most important bits of knowledge that I wish I knew when I first started dealing with TMJ Disorder.
This isn’t supposed to be an academic research paper. I want it to be accessible. It’s meant to be your hack to condense years of googling, scrolling forums, and bouncing from doctor to doctor into a quick(ish) read that can completely change your life - the same way it has mine. You may even have immediate steps you can take to dramatically reduce your jaw pain, if not get rid of it completely.
There’s a reason this thing ended up so long - I actually did the research. And the reality is that there’s nothing simple about the TMJ. It’s part of a complex network of joint tissues, muscles, ligaments, and nerves affected by your teeth, habits, sleep, breathing, facial development, and posture. There are VERY few doctors out there that take all of it into account, so it’s on us as patients to understand as much as we can in order to find the best treatment path.
I urge you to read through everything. You’re dealing with your health here, this isn’t the time to cheat yourself out of knowledge. And most importantly? You have to accept that it’s on you to really understand this thing. Failure to do so is how you get the horror stories of people getting swindled out of tens of thousands of dollars while only making their condition worse. I can promise you it’s going to feel overwhelming at first. But push through - this is the easiest way to save yourself from decades of pain to come.
A Note to Doctors: You’ve probably dealt with a lot of “googlers” who come to you as if they know everything about their disorder. I know you hate it. But let’s think about it from the patient perspective; every practitioner they come in contact with who deals with TMD claims they’re the best. Yet none of them agree on treatment and claim everyone else is doing it wrong. What’s funny is that’s the only thing everyone agrees on - that the vast majority of practitioners in the TMJ space don’t actually know what they’re doing. Meaning from the patient perspective, the chances they go to someone that’s going to fix them is low. The one thing - the ONLY thing - that will help improve their chances is information. Being able to tell, at least from a basic standpoint, what is going wrong in their jaws and whether their treatment plan makes any sense or has any research backing it. To be able to ask the right questions. And to be able to know a scam when they see it. That’s what I want to do here - and I hope you can understand this. Please feel free to comment (if it’s a blog post) or email me with any questions or suggestions. I’m not here to step on anyone’s toes - I just know how hard it was learning all this stuff on my own.
A Note to Everyone: If you find a place where you think I explained something poorly or incorrectly, please reach out and let me know. I really want to improve this ebook, and at this point the only way to do so is with your input.
P.S. This isn’t medical advice
Why is TMJ Special?
Temporomandibular (Joint) Disorder/Dysfunction —or TM(J)D, for short—is a condition that can lead to excruciating pain in the jaw joint area. Along with that pain, many people experience TMJ clicking, sore jaw muscles, tension, stiffness, trigeminal neuralgia, tinnitus, and headaches. Research suggests that up to 30% of the population may be affected by some form of TMJ dysfunction, but closer to 5% suffer pain severe enough to seek treatment.
Unfortunately, TMD treatment is in its infancy compared to other joints. For reference, orofacial pain (which basically just means pain around the mouth and face) was only made a dental specialty in 2020! A lot of this stems from the fact that our medical system is designed to be segmented - meaning there’s a specialty for every system in the body. Unfortunately for us, the TMJ has never fit neatly into a single segment. Think about it. Why weren't joint doctors (orthopedic doctors or rheumatologists) responsible for the jaw joint? After all, the TMJ is the MOST used joint in the human body!
At the end of the day, it’s the fact that it’s so closely linked to teeth alignment and jaw function. Meaning it’s clearly a dental specialty right? Well yes, sort of, except most dentists are lucky to get more than an hour or 2 of class on the TMJ in dental school. Let alone clinical exams or treatment training. Why is that?
It’s because we're dealing with a surprisingly complicated system here. The TMJ is a unique joint sitting in a complex web of ligaments, nerves and muscles. It’s the only joint in the human body that is actually TWO joints mechanically connected. Plus it’s a little weird in the way that it moves (we’ll get into it). And that’s not even zooming in to all the special types of tissues that make up the TMJ - which have dramatic implications on disorder and treatment. Dentists were never expected to take such a deep dive away from teeth.
As silly as it may seem, it was just a lack of clarity for who owns the TMJ; it fell through the cracks. And that’s why we’re left here today picking up the pieces - no standardized treatments, little understanding of the root cause, and complete mess of a system where patients endlessly bounce from doctor to doctor with no end in sight.
Luckily this is improving today. As I said, we now even have dentists being board certified to treat the TMJ. Yet still, plenty of understudied and undertrained dentists will claim they can treat you. To this day, anyone can call themselves a “TMJ Specialist” whether they understand the latest research or not. There are a lot of fantastic practitioners out there to help you… but there are just as many if not more who may actually do more harm than good. Which is why understanding the condition is SO important.
TMJ Anatomy - MUST Know
Alright, here’s the thing. If you’re dealing with TMJ issues, understanding the anatomy of this joint is absolutely essential. I’m not saying you need to become a surgeon overnight, but if you don’t know what’s going on inside your own body, how are you supposed to advocate for the right treatment? How are you supposed to ask good questions, and understand the nuance in the answers? Most doctors, frankly, won’t walk you through this because they’re too busy. So let me break it down for you.
The temporomandibular joint (TMJ) is a marvel of biology. As I touched on earlier, it’s not like your knee, elbow, or shoulder. It’s two joints—one on each side of your face—working in (ideally) perfect harmony. Two joints that are used more than any other in the body, withstanding constant forces from some of our strongest muscles. And this joint doesn’t just rotate like a hinge either; it slides forward and backward in order to achieve full range of motion.
Here’s a visualization of how it moves if you’ve never seen one: https://www.youtube.com/watch?v=nV07g-5u3zE

In this image you can see the 2 phases of mouth opening in the TMJ. First the rotation. Then the slide.
Now, let’s break down the actual components of the TMJ. You don’t have to memorize, but feel free to reference whenever you need a refresher:
-
The Bones:
- The mandible is the entire lower jaw. It’s connected to your skull through the TMJ and a bunch of muscles, ligaments, blood vessels and nerves.

- The condyle (the long part of your mandible that everything rotates around) fits into the fossa (a socket in your skull, right in front of your ear).

- Note that the head of the condyle (which sits in the TMJ) isn’t JUST bone. It’s also covered by a thin layer of what’s called condylar cartilage (we’ll get into it) which is important in preventing wear and tear of the bone.

This image shows that at the very surface of the condyle is a special tissue that helps prevent the forces in the joint from wearing down and damaging the bone itself. In cases of arthritis, this tissue is often worn out.
- The Maxilla is what they call the upper jaw bone. Part of it is the palate of your mouth as well as the upper teeth. It’s fused to the skull, and doesn’t actually move like the mandible.

-
The cartilage
- Articular disc: Sitting between these two bones is a tiny but critical bundle of tissue called the articular disc. Think of it as a cushion that allows smooth movement, distributes forces, all while preventing bone-on-bone contact. Take note because we’re going to be talking about the disc a bunch.
Here’s what it actually looks like in real life! (warning: gross) https://www.youtube.com/watch?v=Nmg3xl13TY0

Notice the different parts of the disc. On the left (back of the TMJ) is retrodiscal tissue (discussed below). In the middle is the disc itself. And on the right is its connection to the lateral pterygoid muscle (used in moving the jaw forward and back).

Front view of the TMJ and articular disc.
- The TMJ has a special kind of tissue inside it that’s pretty uncommon. It’s called fibrocartilage. The disc is actually made of this stuff. And the condyle and fossa have a thin outer layer of it as well. It’s a lot more durable and better suited than other types of cartilage for the grinding and sliding motions of the jaw.

- An important fact about the TMJ’s fibrocartilage is that it doesn’t have nerves or blood vessels running through it. That’s why healthy jaw joints aren’t in pain. Bad thing is that without blood vessels, fibrocartilage doesn’t regenerate. When you wear it down or tear it, it’s practically gone for good.
-
The Ligaments:
- Your TMJ is held together by a network of ligaments. These ligaments don’t just keep the joint in place; they also control how far your jaw can move. If they get overstretched (from clenching, trauma, bad posture, etc), your joint can become unstable (and be able to move in ways that it shouldn’t).



- Although it’s more than just a “ligament”, we’re going to be talking about something called retrodiscal tissue. As you can see below, it’s made up of a bunch of ligaments, loose connective tissue, and elastic fibers. But don’t worry about that. The MOST important thing to take away here is that a large part of this tissue - unlike the disc itself - is FULL of nerves and blood vessels.


-
The Muscles:
- You’ve got a team of muscles working overtime every time you chew, speak, or clench your jaw. The main players are:
- The masseter (considered the strongest muscle in the human body by weight) and temporalis muscles, which force your jaw closed.

- The lateral pterygoids, which control that all-important sliding motion. The lateral pterygoid has 2 heads, one that connects to the disc, and one that connects to the front of the condyle. They actually work in opposites! When the lower muscle is “pulling” the jaw forward, the upper one is “relaxed.” When the jaw is closing—thanks to the big masseter and temporalis muscles—the lower muscle “relaxes” while the upper muscle “pulls” on the disc. This mechanism is important for stabilizing the disc and making sure it doesn’t displace backwards when biting forces are applied.
- The Medial Pterygoids play a part in helping the lateral pterygoids move the jaw side to side, as well as a bit in raising the jaw and moving it forward.

- The suprahyoid muscles, which help with opening your mouth wide, pulling your jaw forward, chewing, swallowing, and breathing

An engineer’s note: These are some of the strongest and most frequently used muscles in the body around one of the smallest joints in the body. Remember from high school how pressure = force/area? We may have a LOT of force. And a very small area. Which is why when things go wrong here, they can go SUPER wrong.
-
The Nerves:
- The TMJ is surrounded by a dense network of nerves, including branches of the trigeminal nerve. This nerve is responsible for sensations in your face, jaw, and even your teeth. When it gets irritated, you can end up with headaches, toothaches, facial pain, earaches, etc.

And look, I get it. This might feel overwhelming. But trust me, once you understand how this joint works, you’ll start to see patterns in your own symptoms. You’ll know why your jaw clicks every time you chew, or why you wake up with a pounding headache after a stressful day. More importantly, you’ll know how to start fixing it. So take this knowledge and keep it close—it’s your first step toward relief.
The Road to Joint Degeneration
I’m not going to lie to you, writing these next sections was HARD. Because there are SO many ideas that are all interconnected. So think of this as an introduction to joint pain. Some of you have experienced this, but many of you haven’t. Either way, it’ll give us a foundation where we can start digging deeper to explain “root causes” and even potential fixes for your condition.
First off, let’s talk about the resting position of the condyle (the part of the lower jaw that sits in the TMJ). Generally, it needs to be centered in the joint. It should NOT rest all the way in the back of the joint socket.


But unfortunately, it’s really common to see people who chronically jam the head of the condyle up and back into the TMJ. For most people, this “jamming” of the condyle into the back of the joint happens when they clench with full molar on molar contact. We’ll get into this more later, but for now, here are some of the consequences:
One, it can put pressure on the “retrodiscal tissue” which, unlike the disc, has a lot of nerves and blood vessels. This can cause sharp joint pain.
Two, it can put extra pressure on the back of the disc, and over time force it to sit slightly in front of the condyle.

And as we mentioned in the anatomy section, when you clench the upper head of the lateral pterygoid “tenses.” That’s the head that attaches to the disc. Meaning over time, this muscle will pull the disc even farther forward.
The disc is thicker in the back than in the middle, so when your disc is forward, its back end can push the condyle back even harder, adding to potential pain.

The shape of the articular disc. You can see it’s thin on the inside and tick on the outside. The outside of the disc also has more nerves
But also, think about what happens when you open and close your mouth. Remember how the jaw joint rotates and then slides? Now when it slides forward it has to POP into the disc! And then if it slides back all the way into its backwards position (fully closed) it’ll POP out. Some of you will recognize this feeling. It’s called “Disc Displacement With Reduction” where reduction just means the disc is able to “recapture” the joint.
If you’re interested, this video is helpful in visualizing all this. Just remember it’s a simplification. https://www.youtube.com/watch?v=mB468Jh9aAY
This is when I started looking into my own TMJ Disorder - when my clicking got bad. But unfortunately for me, google and even the doctors I went to told me that “clicking” isn’t a huge deal and is fairly common. To be fair, they’re not wrong that it’s common. Up to 30% of people experience it at some point! And the fact is that the vast majority of people with joint sounds actually have no pain or extra dysfunction to go with it. But for others, clicking is the signal for the start of jaw joint degeneration. So please take it seriously enough to at least educate yourself. Because here’s what can (but probably won’t) happen next:
Over time, the retrodiscal tissue can stretch more and more as the disc gets pulled forward farther and farther. During this time the clicking may get more violent and loud. It may also get more painful as more of the forces in the TMJ end up being absorbed by the retrodiscal tissue instead of the disc.
At some point, you may start experiencing partial “closed locks” or what they call “Disc displacement WITHOUT reduction” because now the disc isn’t recapturing the joint. This happens because the disc has slipped so far forward that instead of popping into place when you open, it instead folds up in front of the condyle BLOCKING it from sliding forward.
Mouth opening will be limited to around 20mm, and it can be extremely painful. Because remember, now your condyle is fully pressed into the spongy sensitive retrodiscal tissue. And when you try to open, the ligaments holding your disc back get stretched as you push the disc farther forward.

Here’s a good animation of what’s going on: https://tmjtreatment.com.au/what-is-tmj-or-tmd/disc-displacement-without-reduction-3/
Some people are able to “unlock” at this stage. I was able to for several months. I could maneuver my jaw so it recaptured the disc and went back to clicking (I’ll show you how towards the end). But if nothing changes in your posture or habits, this is one of the last times where you can reverse the condition back to “normal.”
The good news is that even if things get worse, you can still regain full pain-free jaw function; it’ll just take some work, and you’ll have to accept living with an abnormal TMJ anatomy (which honestly as long as there isn’t pain or restrictions in opening your mouth, isn’t a big deal at all).
But at some point, you may stop being able to “unlock,” and things get a lot more complicated.
There are still good treatment options at this point, and we’ll get into it in the “treatments” section of the book. But for simplicity’s sake, let’s move forward assuming you ignored all advice and things kept getting worse.
Over time, the retrodiscal tissue and ligaments will stretch and the disc will push forward more and more - which will actually start improving your mouth opening range of motion. Pain may or may not get better too. As time passes, you may start developing scar tissue that starts tying up the different joint surfaces in the TMJ causing more stiffness. They’re called “adhesions.”

Arthroscopic images of “adhesions” in the TMJ. You can see several examples of this webbing of scar tissue going between joint surfaces
But the fact that there’s no disc between the condyle and fossa (lower jaw and skull) makes this the most dangerous time period for TMJ degeneration.
As we mentioned, the masseter is the strongest muscle in the human body by weight. If you’re a clencher/grinder for example, you are now dumping all of that force onto tissue that isn’t intended to support it. Same if you eat super chewy or crunchy foods. Because of this, you’re at high risk of damaging the retrodiscal tissue and tearing it.
Then if you manage to wear down or tear the retrodiscal tissue, you now have bone on bone contact. Which will greatly increase chances of arthritis.

Worn down retrodiscal tissue that may lead to bone on bone contact and arthritis
However, if you manage to eliminate these damaging excess forces from the joint, you may actually be able to recover. That is because as we subtly foreshadowed in the anatomy section, the retrodiscal tissue has a blood supply and nerves. Over several years, this tissue can remodel into fibrous non-vascular tissue people call a “pseudo-disc.” This process can take many years, in which you have to be really careful to avoid high stress on the joint, while at the same time exercising and mobilizing it to prevent unwanted scarring and stiffening.


On the left is a disc displacement where you can see the condyle rides on thin delicate retrodiscal tissue (RT). On the right you see how the back of the disc and part of the retrodiscal tissue has thickened up. It has built up fibrous scar tissue that acts as a pseudo disc.
The exercise and movement is key, because without it the joint will start building up inflammation which will make it even harder for you to move. At some point, scar tissue may even form between joint surfaces worsening the stiffness. We’ll get into some of those mobilization exercises at the end of the book. Avoid extremely chewy or crunchy foods, but don’t put yourself on a soft food diet unless you’re recovering from surgery.
I want to make it clear, I’m not here to fear monger. It’s true that many people live with these mild TMD symptoms that never get worse and no big deal. But whether or not it’s something you can live with, there is no denying that your jaw is dysfunctional at this point. And I just want to make sure that if things DO start getting worse… If the clicking starts getting louder; if it moves to the other joint as well; if it starts locking up sometimes; you’re educated enough on what’s happening; why it may be happening; and what steps you can take to get better. Otherwise, you may regret (like I do) not taking it seriously.
Muscles Are a Big Part of the System
Research shows around 50% of TMD cases involve a muscular component. Although many practitioners in the space will tell you it’s a LOT more. Whether it be pain or tension or both.
For example, as we’ve covered, the lateral pterygoid moves the jaw forward.

What happens when you consistently jam your condyle backwards due to clenching or a retracted mandibular posture? Over time, that lateral pterygoid may weaken, which can lead to a vicious cycle:

Proper mouth opening involves the jaw sliding forward as it opens. A weak lateral pterygoid may not pull that jaw forward properly while opening, leading to more retraction of the jaw, leading to weaker lateral pterygoids, etc. You can tell this is happening when your jaw opens down and back, instead of down and forward. As a result, you use the lateral pterygoid EVEN less which makes it EVEN weaker.
Here’s a video on this topic: https://www.youtube.com/watch?v=3R8vdyFR-mE
On top of all that, you may be clenching/grinding (often without even noticing), which overworks muscles like the masseter and temporalis. And remember, these are the muscles that SHUT your mouth. When they get stronger, and tenser, they only worsen the compression of your condyle into the back and top of the TMJ. Which only perpetuates the muscle dysfunction AND that whole cycle that leads to disc displacement and joint degeneration.
But it’s not just dysfunction. Pain itself can also come from the muscles.
The fact is that the majority of TMD patients experience muscle pain to some extent; many don’t even experience joint pain to begin with. That’s because as any given muscle is chronically overtensed, you can develop what people call [muscle spasms, myofascial trigger points, muscle knots, etc].
These are pinpoint areas of intense pain and tension in a muscle or surrounding “fascia” (pronounced fah-shuh). Fascia by the way is this really thin connective tissue that covers almost every single nook and cranny in your body. It’s also heavily innervated, making it nearly as sensitive to pain as your skin. When stressed, it can tighten; when unused, it can harden; and when inflamed, it can scar.


Sometimes you can literally feel a “knot” which will hurt when pressed. But more importantly, these trigger points can “refer” pain all over your face via your head’s nervous system. This means that you can feel pain in your temples, when the muscle spasm is actually somewhere in your neck muscles. You can feel pain in a tooth, when really it’s just a trigger point in the masseter. Crazy stuff.
Although I won’t lie to you; the scientific understanding of what actually biologically CAUSES these muscle spasms is just not there yet. Three of the theories I’ve seen are:
- It’s a local spot of muscle tissue that lacks the oxygen to change “tone” (muscle fibers need energy to switch from being tense to loose and visa versa). So they’re stuck in a contracted tense state. And produce metabolic waste and acidity that can produce pain.
- It’s a local spot of tightened fascia, which can compress nearby nerves.
- It’s a local site of inflammation in muscle or fascial tissue (from microscopic damage/overuse)
- Dysfunction between where nerves and muscles meet, where the nerves incorrectly overproduce the chemical that causes local muscle contraction
Just note that almost all the things you hear about trigger points come from clinical/anecdotal reports. We don’t have a full understanding of the mechanisms behind myofascial pain. Pain in general is really hard to understand and study actually because it’s so subjective, and the nervous system is SO complicated.
But one of the reasons we’ve seen for muscle tension, discomfort and eventually pain is instability of the TMJ system. Stability just means the joint's ability to maintain its “normal” position and move through its “normal” range of motion.
For example, let’s take a disc displacement with reduction (the condyle pops in and out of the disc). It’s been measured that when the condyle sits inside the disc during opening, muscle activity is normal. BUT, as soon as your condyle clicks out of the disc, there is a spike in activity in your masseter and temporalis muscles - leading to extra tension in order to stabilize the joint in its “normal” position.
Underuse of muscles can also lead to instability. Let’s say the lateral pterygoid (the muscle used for moving the jaw forward) is underused. It may lose its ability to maintain the TMJ’s natural position, and have trouble moving through its normal range of motion (opening your mouth wide). Which means proper jaw motion will strain the muscle and cause pain.
Overuse of muscles is just as bad. For example take a person who mostly chews food on one side. This can be because they already have TMJ pain on one side and want to avoid it, or something completely unrelated to TMJ like tooth pain or bite misalignment. That consistent asymmetrical loading of one side of the jaw can trigger muscle pain. And even worse, asymmetrical chewing can stress the overloaded TMJ and lead to stiffness in the underloaded TMJ. More on that later.
But this is why it’s so crucial to understand that the 2 TMJs are mechanically linked. It’s why asymmetry is extra bad. A disc displacement on one side will cause muscle compensation on the other side. Muscle tension on one side can lead to joint stiffness on the other. It’s a mess.
You also absolutely can’t ignore the instability that can come out of bite problems. For example, you can have bite asymmetry where one side’s teeth touch before the others, which means you’ll have extra muscle and joint loading on that side.
You can also have a misalignment where the teeth don’t fit together comfortably in the position that’s most natural for the TMJ (centered in the fossa). You’ll commonly see, for example, people with underdeveloped upper jaw (maxilla). This will make it so the lower jaw has to sit farther back (recessed) so the upper and lower teeth touch comfortably.

This can be a reason for retracted mandibular posture and why the condyle gets crushed into the back of the TMJ and spirals into TMJ dysfunction and degeneration as we talked about earlier.
But before we move on, let me assure you, you may not necessarily NEED to fix your bite with orthodontic work to fix your TMJ pain. You’ll see how in the postural section.
How do you know if it’s joint pain vs muscle pain?
Normally, joint pain will happen when you’re mobilizing/compressing the joint. Meaning when you open or bite down. It’ll also generally be located right at your TMJ. Which if you refer back to the anatomy section can feel as a little bump right in front of your ear. So if you press on it and feel tenderness or sharp pain - it’s likely in the joint.
Muscle pain on the other hand will feel like a more constant “ache” that you feel around your face - not necessarily the joint area. It may also be referred pain from a trigger point/muscle knot - manifesting as a tension headache, tooth pain, ear pain, or just sharp pain around your jaw area. Referred pain just means the pain you “feel” doesn’t necessarily originate from the same spot you feel it; it could be transported there by a nerve from a completely different spot on your face. You can try to find the trigger points causing the pain by pressing around on your head, neck and jaw muscles for tender spots, which I’ll show more specifically later in the treatment section.
Posture - I Was Tired of Hearing About It… Until I Finally Understood (It was too late)
When I first started digging into my TMD, I read the TMJ subreddit like crazy. We’ll get into what I think about forums and support groups later. But constantly I’d read people saying “it’s all about posture” or “fix your posture” or whatever. Honestly, I hated it. To me it seemed a little “woo-woo” and unscientific. Plus it’s not a very easy fix. It took years until I stumbled on an explanation that managed to tie together the “woo-woo” with the scientific understanding of the joint I already had.
Unfortunately for me, if I had just taken the time to understand this logic when I first started researching my TMJ Disorder, It’s very likely I wouldn’t be dealing with it today. By the time I really started implementing this into my life, I had already developed a permanent “closed lock” on my left side. But hey, I’ve managed to pretty much stop my right side from clicking most of the time, and now live (mostly) pain free day to day. I can’t ask for too much more.
My goal is to tie everything together for you too, hopefully before there’s any permanent damage. But even if there is, there’s still a great chance of eliminating the pain.
Don’t worry, it’s not all about standing up straight
I’m just going to go ahead and tell you the biggest unlock for me that instantly changed the way I lived my life. And actually nearly instantly brought my pain down by half(ish). A lot of it is going to sound familiar. But trust me, the background is much more important.
At the core of it all, is lower jaw posture.
If you look back at the anatomy section, you’ll remember that the condyle sits inside the fossa (your jaw bone sits inside your skull). Sitting between them is the disc. But here’s where a majority of TMJ problems start one way or another.
Something called “retracted mandibular posture.” This is just a fancy way of saying your jaw bone sits too far back in your jaw joint. And here’s why this simple thing can explain so many of your TMD symptoms, whether it’s joint pain, clicking/popping, closed locks, earaches, headaches, you name it.

Figuring out if you’re retracting the mandible
There are a couple ways you can check to see whether the positioning of your lower jaw plays a role in your TMJ Disorder.
The first is by assessing whether your lower jaw is sitting too far back. You can do this like so:
- Close your jaw until your molars touch (they call this “full occlusion”)
- Relax your jaw muscles WITHOUT moving the position of the jaw
- Try to move the jaw backwards
If you can barely move it any further backwards, then you know the closed position of your jaw is causing the condyle to sit too far back in the TMJ. As mentioned, this can spiral into a ton of TMD symptoms you may be familiar with.
Next, is assessing how your jaw is opening. As a reminder, here’s a video you may have already watched that shows difference between healthy and unhealthy opening: https://www.youtube.com/watch?v=3R8vdyFR-mE
Basically you need to recognize whether your jaw moves forward when opening wide, or moves down and back.

On the left you see the jaw moved forward when opening. On the right you see it move down and back. You also sometimes see bulging as a result of the condyle actually popping out of the TMJ a bit. Not good.
If opening with a forward jaw posture feels weird, you’ll need to work on this, and do strengthening exercises of the lateral pterygoids. They’ve likely become abnormally weak. You can find those later in our at home exercises section. But don’t just try to push your opening to be wider and wider if you're retracting the mandible while opening. This produces large shearing forces and is really bad for the joint.
Ok it’s a little about standing up straight…
Forward Head Posture is also a common trait found in people with TMJ Disorders.
If you reference the anatomy section, you’ll see there is a group of hyoid muscles that sit under your chin. These connect your mandible to your neck. You can feel this - the more forward your head goes, the more tension the hyoid muscles exert BACKWARDS and DOWNWARDS on the jaw. You may be able to guess why that’s bad already.
The reason your head moves forward is because at the end of the day, your body HAS to maintain its center of gravity over your feet. Meaning if your shoulders or chest fall BEHIND your hips, the head simply MUST come forward to counterbalance. As a result you get something called swayback posture and forward head posture.

Because this puts backwards tension on your jaw - you’re going to have an even harder time keeping your jaw forward of full retraction. And the extra downwards pressure will make it harder to keep your mouth closed with the tongue at the roof of your mouth. We’re about to go deep on why that’s a problem. And if that weren’t enough, your head is really heavy; the farther off center you put it the less force is distributed through bones (which can handle compression like nobody’s business). Instead, the back of the neck needs to apply a ton of constant tension just to keep it up. That constant muscle strain will quickly turn into a minefield of muscle spasms causing pain all over the head, neck and jaw.

You see forward head posture causing backward and downward forces on the jaw.
The postural “fix”
Exercises are helpful in bringing back stability into the system. You can strengthen muscles that are weakened to help “good” posture feel more natural. They also help mobilize the joint, preventing stiffness and scar tissue buildup. There’s also a lot of coordination that happens between all your jaw muscles every time you open and close your mouth. This coordination is neuromuscular, and will take consistent repetitions to retrain.
But at the end of the day, no amount of exercising will actually bring your posture back to normal. This has to be done by sheer force of will and consistency. Our consciousness and habits can override the body’s postural baseline. Although this is NOT easy. It’ll take 4-8 weeks until you get used to a new posture. At the end of this section I’ll give you a pro tip to make it easier.
But in terms of posture here’s what you need to do.
The key is positioning the jaw slightly forward—just 2-4mm. Lock that into your brain. This might feel unnatural at first, especially since some people are used to their teeth touching when their mouth is at rest. But so often, the bite is a source of the problem. You don’t NEED a “proper bite” to relieve your TMJ problems. The goal here is to gently move the lower jaw forward to take pressure off the back of the joint. If your jaw clicks like mine, you’ll basically want to push your jaw forward JUST past that first click - pretty much forcing the condyle to sit inside the disc.
When you do this, your back teeth won’t touch while at rest, and that’s completely fine. You should keep your lips closed and breathe through your nose. If you do this consistently, the back of the TMJ stays decompressed. It’s fine to have your teeth contact while chewing since it’s relatively a rare event throughout the day.
But a question I had when learning about this: How do you know if you’ve moved your jaw forward too much? And the answer lies in your hyoid muscles. Those muscles just under your chin (refer to the anatomy section for visuals). If you put your finger there, and then slowly move your jaw forward, you’ll notice a point where those hyoid muscles TENSE. That means you’ve gone too far. You should not be using those muscles to keep your jaw forward. Only the lateral pterygoids. If you can barely move your jaw forward without tensing these muscles, it means you have really weak lateral pterygoids and need to strengthen them.

The second most important postural fix is the opening and closing of your mouth. If you remember, it’s all about protracting your jaw while opening (sliding it forward).
Now, here’s where it gets a little tricky—some people have weaker jaw muscles (specifically, the pterygoids, which are responsible for holding the jaw forward). If those muscles are weak, suddenly keeping your jaw in this new position all day can feel exhausting or even make things more painful. That doesn’t mean you’re doing it wrong—it just means you need to ease into it. Some people can keep their jaw protracted all day without a problem, while others may need to start with just an hour and slowly build up over time.
Another thing to note: tongue posture matters a lot. Specifically, it needs to be resting on the roof of the mouth, slightly suctioned. A lot of people will hear this and just place the tip of their tongue right behind their front teeth. This is partially right, but you’ll want to try to get that entire back third of the tongue up onto the soft palate as well.

Here’s a video discussing this: https://www.youtube.com/watch?v=eh9OqEd5z1k&t=218s
It’s important to note that some people may have trouble achieving this because of a tongue tie. Most people have one to some extent; but some people’s tie extends really far up their tongue limiting its mobility. If this restriction prevents you from keeping your tongue at the roof of your mouth, there are some fairly minimally invasive surgeries to take care of it.

You may also have weak tongue, mouth and face muscles that will make it hard to quickly achieve this. I’d look into myofunctional therapy in this case (exercises linked in exercises section).
But for people with weak pterygoid muscles, optimizing tongue posture too soon can actually make things harder. This is because proper tongue posture naturally pushes the jaw back slightly, and if your pterygoids aren’t strong enough yet, it creates extra strain. If you feel jaw fatigue when doing both at once, focus on protracting your jaw first, then introduce proper tongue posture once your jaw muscles get stronger.
For people struggling with jaw fatigue, a simple way to strengthen the lateral and medial pterygoids is by resisting your own jaw movements:
- To strengthen the lateral pterygoid: Place your palm under your chin, gently push down, and open your mouth forward and downward against the resistance. Control the motion on the way back up.
- To strengthen the medial pterygoid: Start with your mouth slightly open. Place your palm on your chin and close your mouth forward against the resistance. Again, control the motion on the way back.


We’ll get into more exercises to help in the at home exercises section.
Finally, teeth clenching during stress, nail biting, extremely hard and chewy foods, mouth breathing, etc, need to stop as well. The nice thing is that jaw clenching habits often stop on their own if you take care of the other posture problems. Because you literally cannot have your jaw positioned forward with a slight gap between your molars AND be clenching at the same time. Clenching/grinding at night is a little harder to control. All those facial strengthening exercises and myofunctional therapy has been shown to reduce nighttime clenching/grinding. You should also avoid sleeping on your back, since gravity pulls your jaw, tongue, and soft tissues back often forcing breathing issues and extra stress on the back of the TMJ. Instead try to sleep on your side.
If for some reason you continue to brux, you should look into a nighttime splint as we’ll discuss in the treatment section.
For resetting your posture, my tip is to set a repeating timer every 20-30min. And set it to vibrate only so it doesn’t annoy everyone around you. https://www.idownloadblog.com/2022/11/23/how-to-set-vibrate-only-alarm-or-timer-on-iphone/
Every time it rings run through the posture checklist:
- Is my lower jaw moved forward those 2-4mm? (While not tensing the hyoid muscles)
- Is my head not leaning forward
- Body aligned? (like we talked about in the previous section)
- Entire tongue suctioned to the roof of the mouth?
- Lips closed?
- Small gap between the teeth?
Over time it’ll become easier and quicker. Until at some point it’ll be your body’s natural resting state. It’s a very difficult, but doable process that as we’ll discuss soon, is worth implementing as soon as possible.
*By the way, if you can’t physically breathe through your nose, you have to look into getting that fixed. I personally don’t have this problem, but the Buteyko Method was recommended (doesn’t hurt to try: https://buteykocenter.dk/en/what-is-buteyko-method/) and otherwise get checked out by an ENT.
The “Root Cause” - Connection to Sleep, Breathing and Development
Now that you understand the surface level aspects of your TMJ Disorder - the anatomy, the posture, even a way to relieve it - we can dive even deeper. To understand how this even all comes about and how it interfaces with sleep and breathing.
In this section, you’ll start to understand why TMJ problems are most common between the ages 20-40, whereas every other chronic pain condition mostly affects older people. And it’s where things really started tying together for me.
Remember all the stuff that happens on the road to jaw joint degeneration? Where your disc gets displaced and can degrade leading to bone on bone contact and arthritis? Well the road actually starts much earlier for many of us TMD patients.
An important note is that most of us don’t go all the way down this road to full degeneration. Instead, they adapt to a dysfunctional jaw early on. And similarly many don’t START getting TMJ problems for the same reasons as others. This is why many will say the “cause” of TMD is unknown. But really it is known, it’s just hard to generalize because of all these systems at play. That’s why it’s good to map out the ENTIRE road of TMD development so you can figure out where you got on so you can figure out how to get off.
The beginning ties back to everything we just discussed about posture.
When we’re growing, our bones are still developing. The maxilla (which is your upper jaw bone consisting of the palette and upper teeth), the mandible (lower jaw), condyle, etc. And bone growth is heavily dictated by the forces applied on it.
For example, the maxilla is heavily influenced by the force applied by your tongue. You may not think much of it, but your tongue at rest appliessimilar forces to those that orthodontists use to move teeth. If applied constantly, this has DRAMATIC effects on bone structure. A lot of doctors explain it like the “scaffolding” of your upper jaw - giving it the structure to grow wide and forward instead of narrow and recessed (as seen in images below). Plus, if you go back to the anatomy section, you’ll notice the maxilla has a big seam down the middle; this seam isn’t even fused until your late teens, making it that much easier for your tongue to widen this bone.


The thing to remember is that your lower jaw “follows” the development of your upper jaw (especially in adolescence). What this means is that as if your upper jaw grows wide and forward, your lower jaw will have room to develop forward as well. But if it develops narrow and recessed, the mandible is forced to sit further back to maintain a functional bite.
So often you see something as simple as allergies, a deviated septum, or really anything that restricts nasal breathing at an early age triggering the entire process. Without nasal breathing, your mouth is forced to hang open to breathe. You physically cannot breathe through your mouth AND have your tongue suctioned to the roof of your mouth, meaning again, an underdeveloped jaw and unstable bite.
Here’s a good video about this (although remember, it’s talking about one potential road to TMD, not all of them): https://www.youtube.com/watch?v=PVxlL_lMces&t=11s
While your condyle is developing, open mouth posture may also impact how your condylar head forms. Specifically, it is normally forced to develop to sit centered in the joint. So think about it, if it develops to be centered while your mouth is open (from mouth breathing), what will happen when you close your mouth? It will jam into the back of the TMJ.

While growing, our condyles are extremely moldable. Which is a very big problem if you’re dealing with that backwards pressure we’ve been talking about. Specifically, your condylar head can shrink and lose its protective coating of condylar cartilage, increasing likelihood of arthritis and in severe (rare) cases something called condylar resorption. In this case, the head of the condyle degrades and disappears. And as the condyle shortens, the lower jaw sits farther and farther back leading to an open bite and lack of “jaw line”. Sometimes this is called “Idiopathic Condylar Resorption (ICR)” just meaning the cause of resorption is unknown. Also it can happen on one or both joints.


Graphical illustration and comparison to MRI of condylar resorption/degeneration. You can see how it affects facial shape on the right
Often orthodontists at a young age will fix the aesthetic issues of the bite without addressing what’s going on in the TMJ. For example, a narrow underdeveloped palette will lead to tooth crowding. That combined with sideways pressure from the tongue when it isn’t resting on the roof of the mouth can lead to flared teeth. It’s insanely common to have orthodontists just pull a tooth and slap on some braces to straighten the teeth. This doesn’t address the root cause, and can often make things worse by conforming a bite to an unstable joint.
Plus if your orthodontist doesn’t actively monitor the position of your TMJ while shifting your bite, they may be forcing the condyle backwards or forwards, potentially triggering more pain and the whole dysfunction cycle. It’s way too common to see people’s TMD problems start in their early teens after getting braces, and then just let it spiral out of control over the next decade because the orthodontist didn’t pay attention to it.
But there’s more… This spiral ties in breathing dysfunction as well. As discussed, Improper tongue placement can lead to a narrow upper palate. But the upper palate is also the floor of the nasal cavity. So a narrow palate means a smaller nasal airway making breathing more difficult. A tongue that sits low in the mouth that has too little space for it will also take up airway space, making it harder to breathe. This may then lead to a forward head posture in an attempt to open up the airway, which can make lower jaw protraction even harder as we talked about. It all feeds into itself.
These resulting breathing disorders then loop into sleep. Snoring and sleep apnea are all linked to this underdevelopment of the tongue, upper airway muscles and palette. The same is true for nighttime clenching and grinding (aka bruxism), which is NOT due to stress unlike daytime bruxism. It’s an involuntary tic that comes from the instability of the jaw and airway.
And of course, once you start clenching and grinding, this is absolute jet fuel onto the fire of TMJ degeneration. Because you’re applying maximum force on potentially weakened or even torn retrodiscal tissue. Especially in developing faces, this force may also speed up condylar degeneration.
You should know that even though all of this is rapidly accelerated in our teenage years, our TMJ structure remains moldable throughout our lives. Bites can still shift. Condyles can still degenerate. And muscles can still weaken. Just remember that this adaptability of the TMJ also means healing is possible, and most of the time actually happens on its own.
But here’s the thing. You’re probably not a child or teenager, and you don’t have a time machine to tell your younger self to do better. Neither did I. Yes, sometimes if you have mild TMD you can resolve it by addressing these root causes. But you have to remember, “once a car is wrapped around a tree, fixing the brake-lines doesn’t matter.” Sometimes the damage has already been done, and you have to focus on fixing it directly.
So in the next 2 sections, we’re going to go over all of the treatment options you have and how to apply them to specific symptoms. There’s still plenty of time to fix things.
Treatment Options
I really want to make it clear that I’m not a doctor. And none of this is medical advice. You should absolutely find yourself a doctor who will help you regain your jaw health. But… BIG but… the TMJ world is littered with doctors who flat out don’t know what they’re doing. Doctors who will gaslight you. Who will not listen and will not be able to explain anything. They will charge you an arm and a leg for treatment - with no guarantee. And sometimes just make your condition worse.
Hopefully the biggest thing you get out of this section and document in general is the ability to figure out which doctors really have your best interest at heart - and which are completely BS’ing you to get your money. After reading this, you’re going to have so many more questions than when you came in. That’s a good sign that you’re learning something. And now you’ll know exactly which doctors to avoid when they can’t explain it.
Something that generally most doctors will agree on is that because it’s SO hard to pinpoint the root cause, and many treatments have not so great success rates (plus it varies highly from doctor to doctor), you’ll want to start with the most CONSERVATIVE treatments, and work your way up. They’ll often say the last option should be surgery. Because at the end of the day, over 90% of TMD cases resolve either on their own or with conservative treatment methods.
But there’s a lot of nuance as to what’s “conservative.” So I made a list of all the major treatment options available to you, as well as my opinion as to their risk and reward levels (with explanations).
Diagnostics/Imaging
LOW Risk, HIGH Reward
This isn’t technically a “treatment” but it’s a good idea to get some diagnostics done as a part of the process. You’ll mainly want to understand if you have structural problems with the joint as opposed to just muscular ones; because there have been plenty of cases where people are walking around with bone on bone contact and arthritis without even knowing it - and just as many with pristine joint health experiencing crippling pain.
You’ll need to go to a “TMJ Specialist” for this. Most use CBCT scans, but sometimes you’ll get an MRI. If you’re curious, the difference is that CBCTs are way more available and cheaper than MRIs. But they’re not able to visualize soft tissues and inflammation like an MRI can - mostly just the bones, their positions, and any arthritic changes to their structure. So if you’re trying to image a disc displacement, you’d need an MRI. Otherwise, a CBCT works perfectly.

Here’s what a CBCT can show you; great at visualizing bones.

And here’s an MRI where you can see the disc.
I found these videos to be really helpful in understanding my own MRIs and just visualising all the different TMJ Disorder problems. You can literally request the MRI notes or images from your doctor (looking at your own MRI images can be really cool, I recommend it) and end up understanding everything they say! Make sure to have google handy though since they use a bunch of radiology jargon you’ll have to look up.
https://www.youtube.com/watch?v=H8VEsxqYxx0
https://www.youtube.com/watch?v=Pb77lR2k_fU
But remember, ANYONE can call themselves a TMJ Specialist. There are some fantastic doctors who have dedicated their lives to helping people with TMDs. But there are more who call themselves experts after taking a one weekend long course. It may take time to find one that genuinely does the research and listens to you.
My advice is to find a board certified orofacial pain specialists - which as of 2020 are officially the 12th dental specialty. There aren’t that many yet - and as with any specialty there are good ones and bad ones. But at least there is some standard.
Here’s a website where you can search for ones in your state: https://aaop.clubexpress.com/content.aspx?page_id=2720&club_id=508439
But I personally got my first diagnostics from my local university hospital from a maxillofacial surgeon. You don’t have to make it hard on yourself. Just make sure it’s someone who has credibility in the space and good reviews - at the end of the day, what you’re really looking for is more information to lead to better treatment decisions later on.
Postural Changes
LOW risk, HIGH reward
As we discussed, this is not only free and something you can start working on today, but it also potentially has the biggest impact on your TMJ symptoms.
Of course, it’s not going to grow back bone or dissolve scar tissue - but for anyone in earlier stages of disorder this may be your key to prevent getting worse. But even for people in later stages, living pain free day to day is not out of the question. This is an option that should, in my opinion, ALWAYS be tried seriously before spending a ton of money or taking on invasive surgery.
Physical/Manual Therapy
LOW+ Risk, HIGH Reward

In physical therapy, you’ll combine massages, mobilizations, stretches and exercises of the TMJ system, which has been studied to have really positive effects on range of opening/mobility and pain levels.
Honestly, this is one of the first things you should do - find a specialist (PT or other) to teach you all the at home manual therapy and exercises and make it part of your routine. The reason it’s in a “LOW+” risk category is simply because you’ll have to pay a decent chunk of change per visit (often uninsured) - and you may not be able to find a competent practitioner around you on the first try. That’s why I always recommend educating yourself first for free.
But seriously, there are endless reasons to implement PT into your life. Movement is CRITICAL in preserving joint health, and helping the TMJ system adapt to change (something it’s really good at if you let it). For example, lack of movement has been shown time and time again to lead to higher levels of joint stiffness, inflammation, and scarring. Improper movement, Asymmetries, and muscle strength imbalances can also be taken care of with consistent repetition of specific jaw exercises.
I’ll share some you can try in the at home exercises section.
Thermotherapy
LOW risk, MEDIUM reward

From a TMJ Association poll, 74% of TMJD patients felt relief from a warm/cold compress. Generally, you’ll want to use a warm compress when the issues are muscular and a cold compress when it’s joint inflammation. But honestly, most of the research for cold aiding inflammation refers to short term inflammation (like bruising). Not much for chronic inflammation. But either way, it’ll feel nice during a flare up. Do avoid cold when it comes to muscle tension and pain from muscle spasms (trigger points) since cold constricts blood vessels and increases muscle tension.
There are a couple of reasons for why hot/cold can help manage pain.
The first relates to how pain works fundamentally. Your skin has temperature sensing neurons.(thermoreceptors) And there are a couple theories as to why (pain gate theory, neuromatrix theory of pain, etc.), but it’s been extensively shown that activating these thermoreceptors blocks perception of pain from that area. In other words, extreme temperatures “interfere” with pain processing which leads to relief.
Heat also helps by dilating blood vessels, boosting local circulation, flushing out painful metabolic by-products, and re-oxygenating muscle tissue. It also increases collagen flexibility, reducing muscle tension and spasms to improve mouth opening, jaw function, and even bite force when combined with light massage. Because it’s applied directly to the trouble spot, it avoids systemic drug effects, though it requires consistent use and proper setup to work—and should be avoided if there’s acute inflammation or injury, in which case cold therapy is preferred.
Sometimes you’ll hear that “wet” heat is better than “dry” heat. But studies mostly confirmed that the difference is negligible, especially because your skin produces sweat anyways.
What’s more important is the “stickiness” of a therapy, meaning how likely you are to continue using it for a long period of time. So do whichever is most convenient and feels most comfortable.
Important Note: This is a good way to manage pain and tension day to day. But it’s not actually a root cause treatment. You’re not going to fix any of the reasons for why you’re experiencing the pain in the first place.
Self Massage
LOW RISK, MEDIUM Reward

50-80% of those with TMJ disorders are estimated to experience muscle tension or pain. As we discussed, the root cause is usually imbalances and compensation - but the result is tons of muscle spasms (trigger points) that refer pain all over the face.
Similarly to thermotherapy, self massage is one of the most effective at home tools you have to manage this on the day to day. It should become part of your routine. But it’s not actually going to cure you.
Same way you have thermoreceptors, you have mechanoreceptors that block pain in a similar way when activated. This is why you’ll instinctively start rubbing the spots that hurt. Vibration for example will act in a similar fashion.
But even more importantly, massage has been shown to improve mobility, reduce muscle tension, and even help release muscle spasms that may be causing prolonged pain.
The thing is that there are specific places you have to massage and special techniques to do them (rubbing where it hurts isn’t going to cut it). That’s why In the last section I’ll go over and teach you the BEST ones you can start using ASAP.





Pharmacology
LOW Risk, LOW reward

This includes off the shelf NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) like ibuprofen or aspirin, prescription anti-inflammatories and muscle relaxants, and supplements like magnesium glycinate. This is by far the most common treatment people start out with. Just remember, this is just another way to mask pain and slightly reduce inflammation; not a root cause solution, but can definitely be useful for symptom relief when the flare ups are at their worst.
Massage Therapy
LOW+ Risk, Medium Reward

Going to a TMJ specialized massage therapist can feel really relieving when it comes to muscle pain - for the same reasons we talked about in the “self massage” section. It’s not exactly working towards a fundamental cure of your disorder. But hey, sometimes it’s not about the cure - it can be about feeling better for a bit and that’s all right.
The reason it’s “LOW+” risk is because learning the right self massage techniques is free - while going to a massage therapist definitely isn’t. If you have the money, go for it! If they know what they’re doing, the massage will be much more effective. Just know that it’s a skill you can teach yourself if money is tight.
Chiropractic
MEDIUM Risk, Medium Reward

I’m not going to lie, I’m personally very weary when it comes to chiropractors for TMJ. I’d say heavily avoid any that will do extremely hard and fast adjustments on the jaw joint. It’s very delicate, and trauma is a great way to instantly stretch/tear ligaments, break bones, and induce unnecessary inflammation that can lead to scarring. These forceful adjustments aren’t worth the risk, since at best they’re as good as slow controlled exercises/mobilisations, and at worst can cause irreversible damage.
To be fair though, “chiropractic” is a general term; there are plenty of really good knowledgeable chiros out there. Many will teach you manual therapy techniques similar to what you’ll find with good PTs and massage therapists, which is totally fine. And plenty of TMD patients find relief there from light manual adjustments plus machines like lasers, red light, acupressure, ultrasound, shockwave, etc. that some chiros can have in office.
BUT the main reason you should be weary is because chiropractors are by far the most business savvy practitioners you’ll find. They WILL try to sell you on a long “treatment package.” Many will claim they can cure your TMD if you pay for 12 sessions - with no guarantee that you’ll feel any better in the end. They’re just way more likely to be more salesy and costly and unscientific than somewhere like a PT clinic. Because there’s just so much more money in chiropractic, so the incentives drive for better salesmanship.
Again, this of course varies from chiro to chiro - but it is a pretty clear trend I’ve noticed over the years.
Also, some won’t work on the TMJ, but will try to convince you it’s actually because you have a misaligned spine or something. This is a classic case of a hammer thinking everything is a nail - and it’s nonsense.
All in all, the risk is higher because a bad one can injure you, and the vast majority will cost a lot of money for some pretty hand wavy treatments. But of course, if you already know a good one, go for it.. Just saying it’s not the safest FIRST place to look for treatment.
Dry Needling
Low+ Risk, MEDIUM Reward

I personally haven’t tried it, but dry needling may be helpful for muscular TMJ problems. The goal of dry needling is to get very fine needles down into the muscle tissue around potential trigger points, and then even wiggling them around a bit to stimulate a “twitch” response.
This is another way to promote blood flow to that specific area to stimulate healing and reduce tightness.
This isn’t going to be a foundational treatment for the TMJ Disorder, but it may help you deal with the pain and tension that comes with it as long as you’re okay with the cost. It’s at a Low+ risk because you can just go try it once and see how it goes, there isn’t usually too much pressure to sign up for an expensive treatment program up front.
Botox
Medium Risk, Medium Reward

I really wouldn’t recommend getting botox from someone who isn’t specialized in treating TMJ disorders with it. In reality, botox is needed a lot less frequently than it’s portrayed to be.
The risks can be injecting the incorrect muscles, injecting nerves, and even destabilizing an already degraded joint and making the pain/damage worse. It’ll also cost you to keep reinjecting every couple months.
To be fair though, the effects are temporary, and it may really help with daytime and nighttime jaw tension/clenching, and lessen pain stemming from the masseters.
At the end of the day if done by someone who knows what they’re doing it’s not very risky. If you have the money you can try and see; a lot of people say it helps.
Arthrocentesis
MEDIUM Risk, MEDIUM Reward
This is usually the first surgical procedure to be considered when there’s structural joint problems that won’t go away with conservative methods.
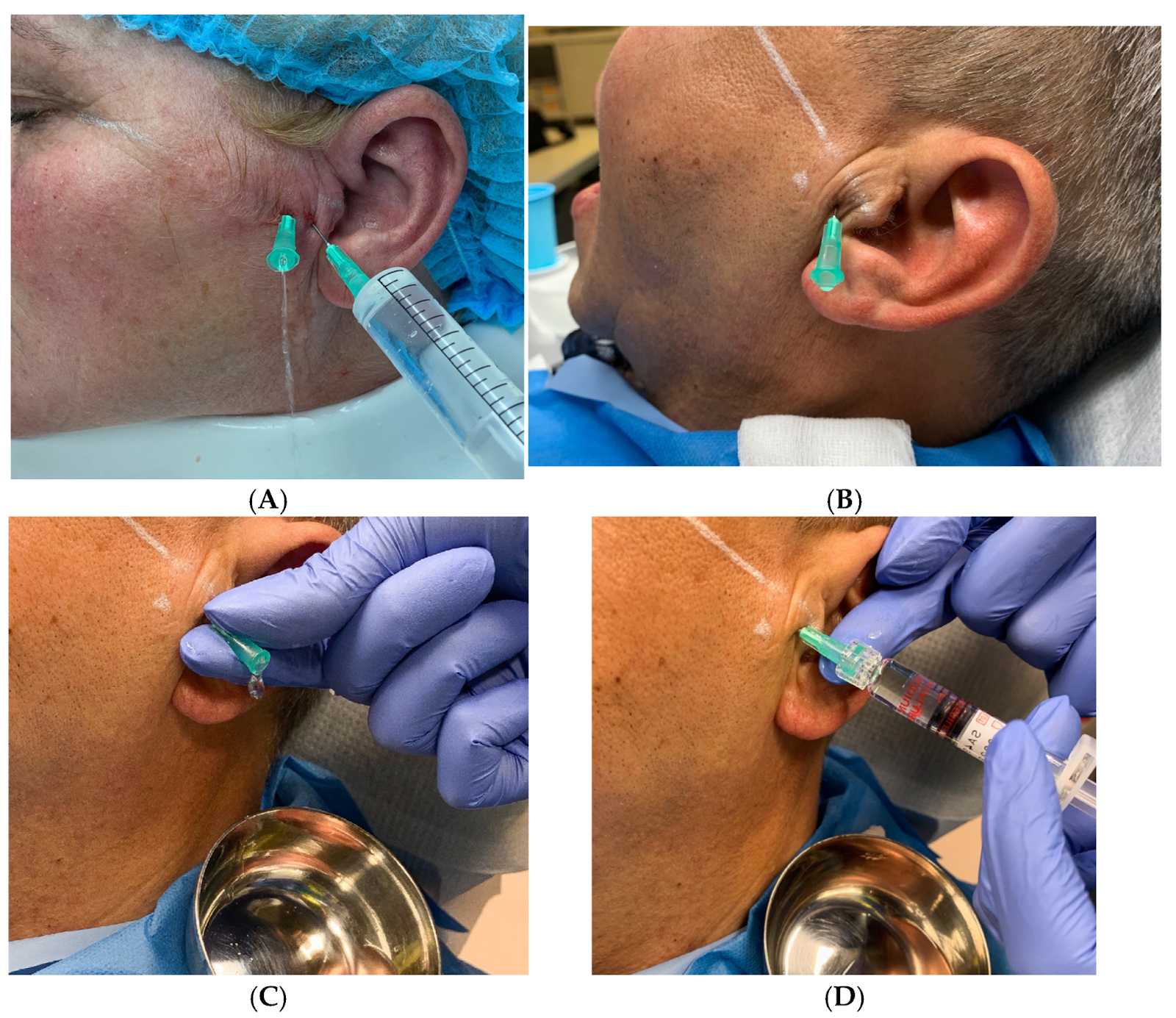
It’s by far the most conservative surgical procedure out there, where they poke 2 needles into the TMJ to wash it out (lavage). Although sometimes they’ll just use one needle to “pump the joint” to try to free the disc with a bit of pressure.
It’s also common for them to place a steroid into the joint, which helps reduce inflammation.
This procedure has shown success in reducing symptoms in a significant number (80%+) of patients, and is thought to wash out some of the fluid build up that produces chronic inflammation and pain. Usually it’ll be followed by PT, as are all surgical procedures we’ll discuss moving forward.
Arthroscopy
MEDIUM+ Risk, MEDIUM-HIGH Reward
This surgery is gaining a lot of popularity in the TMJ space - and its biggest plus is how non-invasive it is. The idea is they make a super small incision, and use little probes called arthroscopes to visualize and manipulate tissue in the TMJ. There are 3 levels of arthroscopy based on how many of these arthroscopes you use.

A level 1 arthroscopy is mostly diagnostic, because there’s only one arthroscope with a camera attached to it. It’s helpful in seeing how damaged different parts of your TMJ are, and is often combined with Arthrocentesis to try to flush out the joint. The surgeon can also use the arthroscope to push around on the joint to mobilize it, making it very successful at reducing symptoms and improving range of motion without necessarily repositioning the disc.
Advanced arthroscopies (level II and III) are ones where you insert 2 or even 3 probes into the TMJ that can actually start manipulating things like the articular disc, cut away scar tissue that’s limiting mobility (adhesions), and fix inflamed tissue by zapping it with high energy radio frequencies (coblation).

(a-f) things surgeons look for during a TMJ arthroscopy: (a) Retrodiscitis (b) Adhesions (c) Small disc tear/perforation (d) Large perforation with condyle visible (e) Villonodular synovitis (f) Polypoid synovitis
After being combined with PT, you’re looking at around 70-90% success rates in reducing pain and improving range of motion.
The biggest risk with arthroscopies is that even though these probes are minimally invasive, you’re still dealing with a very small and sensitive joint. By putting any foreign objects in there, and especially with any manipulation, you’re increasing the likelihood of creating extra inflammation and scarring. So this is still something you want to avoid if you’re early into the disorder, and should only be attempted after conservative treatments have failed. But it’s also why taking recovery PT seriously is so important - movement is your best friend when it comes to preventing the joint from stiffening up post surgery.
Also cost wise, they can get quite pricey if not covered by insurance. Although these days, especially if you get them in university hospitals, some insurance does end up covering surgery. Worth figuring it out if you get to that point.
I really want to make it clear that arthroscopies should pretty much ALWAYS be attempted before open joint surgeries. And even when a level 1 arthroscopy fails, you should try to find a surgeon who performs advanced arthroscopies before moving on to opening the joint. They’re dramatically less risky.
Splint Therapy
MEDIUM Risk, MEDIUM-HIGH Reward

Splints get a LOT of hate in the TMJ world, mainly because there hasn’t been many research studies showing their effectiveness. But these orthotic appliances are NOT all the same. And neither are the specialists who prescribe them.
They’re a removable dental appliance that sit on some or all of your upper or lower teeth. Typically a dentist will custom mold one for your teeth, and then fit it and readjust it. Some are recommended for night time use only, while some are worn throughout the day.
Fundamentally, splints are just mechanical ways to change your lower jaw posture. In theory, this is gold. Think about everything we talked about in the posture section. If you can find a specialist that really knows what they’re doing, really listens to you - it can be well worth the money.
For example, if you have a disc displacement, some splints have been shown to help reposition the condyle back under the disc. Even if this repositioning doesn’t happen, a splint can help reduce the loads on the retrodiscal tissue to allow it to safely grow fibrous scar tissue without degenerating. That’s important because this tissue is much more durable than regular retrodiscal tissue, and doesn’t have any nerves or blood vessels. This means once you take off the splint, you can use the joint pain free.

Image showing fibrous scar tissue forming in the retrodiscal tissue that mimics similar behavior to a disc
Certain splints can also help stop bruxism (nighttime clenching/grinding) if it doesn’t go away on its own from postural changes or myofunctional therapy. This can mean everything for preventing further joint degeneration and giving it time to adapt without all those extreme forces.
But in practice, this is not easy to accomplish and has major risks that have created countless horror stories that tarnished the industry’s reputation. So make sure the doctor you choose isn’t putting you under these risks.
The NIH recommends you don’t use splints that change your bite permanently. Because the potential damage they can cause vastly outweighs the benefits. This includes splint therapy programs that aim to permanently shift your jaw forward or backwards, or even splints that only cover SOME of the teeth (some only cover the front teeth for example) because they will shift the teeth they sit on.
If you experience pain because of it, stop wearing it. If you start clenching/grinding because of it, stop wearing it. Bring it back to your doctor and make sure they listen to you (often it just needs a readjustment), because these can be signs you’re making things worse. But basically just make sure that if for some reason the splint changes your bite, it’s not intended to do so permanently, is not worn all day every day, and isn’t prescribed for prolonged use (over 6 weeks).
There’s also the financial risk. There are many many specialists out there that will charge tens of thousands of dollars for their “protocol.” These are usually the ones that promise permanent changes to the bite. These are HIGH risk. Just find someone else that won’t risk irreversible damage first for cheaper.
Orthodontic Treatments
HIGH Risk, MEDIUM-HIGH Reward

We talked a lot about how an unstable bite may have been the cause for chronic retraction of the condyle and a bunch of these TMJ issues. So why isn’t orthodontic treatment #1 on the list? Shouldn’t we fix the bite and then tadah no more TMJ dysfunction?
Well in a magical risk free world, the answer would be sure. But unfortunately there are some very good reasons to avoid orthodontic treatments until other options fail. Because the truth is that artificially shifting a bite in a way that correctly positions the TMJ is extremely difficult even if you’re trying - where many orthodontists actually don’t pay much attention to the TMJ in the first place. Even with good splints, it’ll sometimes take a couple adjustments to get rid of your pain. You don’t have a couple tries with braces. You have one very long and expensive try. The risk of your doctor not being up for it is just too high. And braces weren’t designed for the millimeter accuracy needed in aligning the TMJ.
Plus, the reality is that most people with an “imbalanced bite” don’t even have TMJ problems. So if your main goal is to reduce jaw pain, you’re better off just applying the postural corrections we talked about first which just get you to avoid full molar on molar contact anyway.
And if you really can’t manage to implement any of the conservative methods, you’re still better off just getting a splint to temporarily fix your bite instead of risking an irreversible mistake.

On a different note, one orthodontic treatment that has been getting more and more popular is palatal expansion. This is where in the case your maxilla didn’t develop wide enough they fit in an appliance that sits at the roof of the mouth and applies a bunch of force to, well… expand your palate. This will cause permanent bite changes (as is intended) that may indirectly help TMJ Disorder. It has also been shown to improve sleep and breathing disorders (which sometimes helps eliminate bruxism); and of course improvement of aesthetics of the teeth and jaw. If you’re someone who clearly has an extremely narrow palate and all the symptoms trickling down from it, palatal expansion may be a good fit. But if you’re not a severe case and the main goal is to just reduce TMJ pain, you’re better off going with more conservative methods.
Invasive Surgeries
HIGH+ Risk, HIGH Reward

Invasive surgeries should only be considered once all else fails - especially if there is just too much degeneration of the condyle. Because no joint that is surgically entered can be expected to function again as normal. A certain amount of scarring and restricted movement almost always occurs. There’s also a small risk of damage to facial nerves.
Not all open joint surgeries are the same though. Here are some of the types:
Arthrotomy: A procedure where the surgeon opens up the joint to reposition the disc, or shaves down bone affected by arthritis, or any other alteration to joint structure.
Total Joint Replacement: The surgeon cuts away the components of the TMJ (all of which are damaged at this point) and replaces them with a prosthetic.

Orthognathic Surgery: This is used to correct extreme jaw abnormalities like heavy under-bite, overbite or asymmetry. Surgeons cut the jaw bones and reposition them using plates and screws.


Invasive TMJ surgeries used to have insane re-operation rates (like 50%) but luckily TMJ surgeons have gotten better over the years and pushed success rates higher and higher to 90%+.
Symptoms, Explanations, and Recommendations
Jaw Pain
Generally, most pain can be categorized in to joint pain or muscle pain
The best trick to distinguish between the 2 is by testing how the pain is triggered.
Joint pain is usually a sharper pain directly on the TMJ (you can find it as the little bump directly in front of your ear; check the anatomy section for reference). It’ll be triggered more through movement, direct pressure on the joint, or compression of the joint. So put your hand on your chin and lock it in place while resisting opening, closing and side to side movement of the jaw. If that triggers most of your pain, it’s more likely to be joint related. You can also put a little pressure on the TMJ to test whether that’s where the pain is coming from.
Muscle pain on the other hand will feel much more dispersed across your face. This is usually caused by what practitioners will call muscle spasms, muscle knots, or myofascial trigger points, which can refer (send) pain all over your head, neck and jaw. You can feel around for these spots by pressing into different muscles - when you feel the pain light up, you know it’s muscle pain. It can also just be general muscle soreness or a fatigue feeling as well.
Additionally there are cases in which certain nerves, usually stemming from the trigeminal nerve, get compressed - which can also lead to chronic jaw pain, ear pain, and even sensation of tooth pain.
For muscular pain, we talked about a bunch of conservative ways to deal with it, including heat (cold tenses muscles and limits blood flow), massage, NSAIDs, at home manual therapy, dry needling, botox, etc etc. These will be your friends day to day, but try not to get stuck in a “painkiller” mindset. Usually muscular dysfunction stems from the root causes we talked about earlier.
For both this and nerve compression, you’ll really need to implement the postural corrections (discussed in postural section) and exercises (at home manual therapy section) talked about in this book if you want a chance at a permanent fix.
For joint pain, you can also use thermotherapy (use cold if there’s heavy inflammation) and NSAIDs for day to day pain management. I would also stop eating any super hard and chewy foods immediately BUT DON’T go on a complete soft food diet (unless instructed by a doctor for a short period). Movement is extremely important for joint health - if you completely stop it’s only going to make things worse long term. Which is why you’ll also want to really focus on daily joint mobilization exercises - which have been shown to reduce pain, improve mobility, and decrease stiffness in the joint.
You’ll also want to cease any clenching/grinding whether it’s daytime or nighttime. If postural corrections don’t help, look into a splint.
Joint pain is a little more dangerous than muscle pain generally speaking. I’d recommend going to get some diagnostics done. You want to know how bad of shape your joint is to decide how much time you have to experiment with conservative measures. For most people though, you’ll quickly discover the joint degeneration is in its early stage. For example if the worst sign of joint dysfunction has been clicking, or infrequent lockups, you don’t need to worry about surgery yet. Just focus on making those postural changes and get your physical therapy exercises in. Then slowly make your way up the “risk” levels we discussed.
But if your joint is already pretty far into degeneration with arthritis or severely limited opening (and none of the conservative methods have worked!), I’d look into those arthroscopies. I can’t hit home enough the fact that just because your joint is in bad shape DOES NOT mean you need to live in pain.
You can have people with absolutely obliterated joints walking around pain free day to day, as well as someone with perfectly healthy TMJs crippled by pain. We’re still trying to figure out the biological mechanisms and layout of everything inside the joint - and something as complex as pain just isn’t predictable yet. But this is actually great news for you - it means there’s a way to live your life pain free whether or not you have healthy jaw joints. This has been shown again and again in research. So keep your head up!
Clicking/Popping aka Anterior disc Displacement WITH Reduction
The clicking/popping sounds coming from the TMJ is called disc displacement with reduction. That is because, as you’ll notice if you have it, you hear 2 clicks when you open and close your mouth: one when you open, and one when you close.
This is due to the articular disc being slightly displaced in front (anteriorly) of where it should be, so your condyle pops IN and then OUT of that disc as it slides forward and back. The fact that the disc is recaptured is called “reduction.”
This is one of the most common symptoms in TMJ Disorders. Up to 30% of the population experiences it! But even though it’s common and often doesn’t come with any pain, it doesn't mean it’s normal. It puts your joint in a more compromising position; most people’s TMJ dysfunction isn’t bad enough to counteract the body’s ability to heal and adapt to the new structure; but if you’re one of the people who constantly overloads the joint for whatever reason - clicking may just be the first stage in the cascade to further joint deterioration.
A brief glance at the cascade: https://www.youtube.com/watch?v=mB468Jh9aAY
Because you’re more than likely to live pain free without too many limitations, the best treatments at this stage are the super low risk ones. I actually managed to eliminate the clicking on my right side (after 4 years) during the daytime with what I learned in the postural section. There are also some specific exercises and muscle releases that help with the clicking as we’ll show in the next section.
If none of that helps and the clicking is really bothering you, some specialists have shown success in recapturing the disc using a splint that keeps your jaw in a more forward position. The goal is to also build up some fibrous scar tissue behind the disc so your condyle doesn’t ride on sensitive retrodiscal tissue, and a splint may help achieve that without risking damage to the retrodiscal tissue. But there are risks as we discussed in the Splint Therapy portion of the Treatment Options section.
If you have bruxism that doesn’t improve, it may be smart to find a nighttime splint to put an end to it.
Closed Lockjaw or Anterior Disc Displacement WITHOUT Reduction
As we’ve touched upon in previous sections, when the articular disc stretches farther and farther in front of its correct position, it may fold up or get trapped in front of the condyle. At this point, it can block forward motion of the TMJ completely - which will feel like a closed lock.


This can happen as over time, your condyle puts pressure on the back of the articular disc pushing it forward and/or the upper head of the lateral pterygoid (which is connected to the articular disc) pulls the disc forward. Remember, the upper head of the lateral pterygoid muscle contracts when you CLOSE your mouth, so this can be exacerbated or triggered by clenching, grinding, chewing, etc.
Generally, when a close lock happens the first couple times, you’ll be able to unlock it with manual manipulation. Here’s how:
- You’ll want to make sure as much tension as possible is released from the lateral pterygoid (which pulls the disc forward) and the chewing muscles (masseter and temporalis). Use heat and the releases you’ll find in the at home manual therapy section. Then just make sure to consciously relax your jaw as much as possible.
- Move your jaw sideways AWAY from the locked joint as far as possible.

- From that position, open your mouth as wide as possible.
- From the sideways open position, move your jaw back to center while still opening wide
- Repeat several times if it doesn’t work immediately
If this doesn’t work, you can also try this:
- Lay your index finger on top of the bottom molars on the side with the lock. Meanwhile, place the thumb under your chin.
- The goal is to push down on the molars and up on the chin to create space in the joint. You’ll feel a light stretch, but don’t push too hard to where there’s pain.
- Then use your jaw muscles to slowly move the jaw forward. It may help to move it sideways away from the locked joint as well. Keep movements slow and controlled.
- Try to hold this force for 20-30s if it doesn’t instantly click.
If you’re able to unlock, slowly close your mouth to a position where your jaw is protruding forward and your front teeth are touching. Then you can relax for a few seconds and try to open wide and then return back to the front teeth touching.
If this works for you, I’d recommend trying to get a splint that positions your jaw forward ASAP. It may take a couple days for the disc to settle back in place, and you need to avoid clenching on the back teeth at all costs which would likely re-dislocate the disc. And if you don’t have access to a repositioning splint, during the day just try to keep your mandible pushed forward that 2-4mm we talked about in the postural section. And at night, try to sleep completely on your side or else you’re more likely to lock up at night. You can probably look up methods to not sleep on your back.
If you weren’t able to unlock, try to find a TMJ specialist in your area that can unlock a closed lock. Sometimes they’ll even pump the joint with sterile fluid a bit to lubricate and loosen it up. And of course they’ll have a better manipulation technique than you.
Timing is CRITICAL here. It’s still really likely unlockable within the first couple months. So do everything you can to visit as many specialists as you can during that time frame. Some will not even try to unlock you.
Because after a long enough time or many lockups, it may become impossible to reduce the disc in this way. It could be because the disc lost its shape (it should be thin in the middle and thick on the outsides), so it can’t hold itself on the condyle as well. It could be because the retrodiscal tissue has stretched too far to hold the disc from slipping forward. It could be because the disc folded up in a weird way. Or it can be from scar tissue build up over time that glues the disc in place.
Don’t worry though, all is not lost. The TMJ is actually a really adaptable joint. It’s been shown that the vast majority of patients who experience a “permanent closed lock” can actually end up regaining normal joint function fairly quickly.
While the articular disc itself can’t really heal, the retrodiscal tissue is full of blood vessels. Over time, with consistent exercise and mobilization that retrodiscal tissue will stretch and grow fibrous scar tissue similar to what the disc is made of (some people literally call it a “pseudo disc”). As a result, you’ll likely develop nearly perfect joint function with no pain.
But you need to be SUPER careful at this stage. It takes time for the pseudo disc to form, and once it does, it’s only around half the strength of the original articular disc. If you haven’t taken care of your clenching, or anything else that’ll cause extreme loading on the joint, that retrodiscal tissue will wear down instead of thickening. So you need to be extra serious about developing good posture and habits to prevent degeneration, along with joint mobilizations and exercises that prevent scarring and inflammation.
It’s also worth looking into arthroscopies. You may have developed some inflammation and scarring in the joint that’ll make healing and movement harder than it has to be. In some cases, advanced arthroscopies can even help reposition the disc. But at this stage you’re still FAR away from needing open joint surgery, you don’t NEED the disc in the right place for painless jaw function.
Open Lockjaw (Subluxation of the TMJ)

This is a scary one. But it’s usually less dangerous than a closed lock in terms of joint health.
What’s happening is one way or another, your jaw gets pulled further forward than it should.
Specifically, the condyle can get pulled past what’s called the articular eminence (the bony bump in front of the TMJ that usually acts as an endstop). Once the condyle makes it over the eminence, your muscles can’t produce a backwards force to get it back into position. They just pull harder into the bone.

You can see how you don’t actually have any muscles that are able to pull the jaw down and back once it gets over the hump
All you have to do is push your mandible down and back to reset it. Someone else can push down on your molars with their thumbs while pushing your mandible back. Or you can do it yourself by putting your index fingers on the molars and thumbs under your chin - while pushing down and back.
Here’s a video to show it: https://www.youtube.com/watch?v=xVvO_tl0w_w
Then, just try to avoid opening wide enough for this to happen. Your ligaments may just be more stretchy or loose than they should be, or maybe you have a smaller articular eminence. If you can’t reposition the jaw at home, visit the hospital.
Crunching Sounds in the TMJ

Obviously I can’t diagnose you over written descriptions of sounds, but if you’re feeling more of a crunch rather than clicking, you may have already entered the state of bone on bone contact (without the disc in between). Definitely get some scans done.
As I’ve said, your goal is to avoid needing a joint replacement. In this case, it may be worth leaning into a softer food diet if possible, and of course classic postural work and physical therapy. Again, even without a disc, it’s very possible to live without TMJ pain.
Mainly, your goal should also be to eliminate any high loads, especially from clenching behaviors, whether it’s through postural work, botox, splint therapy, etc. You no longer have a disc to distribute the forces generated by your masseter (they generate a LOT of force). The second priority should be to do your manual therapy exercises to minimize inflammation and further bone degeneration. I can’t overstate how important movement is to joint health.
If you’re going to need surgery, look into arthroscopies first to clear out any scar tissue and inflammation that may be limiting mobility. Only once your joint is completely deteriorated will you need a total joint replacement.
Limited Opening (Not due to disc Displacement)
This may be due to a couple things.
- It could be due to the mechanics of how you open your mouth. If you’re not moving your jaw forward while opening, you may be crushing your condyle into the back of the joint, which prevents it from achieving the joints natural range of motion (much of which it gets from sliding forward). No amount of exercises is going to improve this. In fact it will make it worse. It’s a mechanical issue, so don’t force it… fix it. Read more about this in the posture section.
- It could be from things called adhesions. Basically this is scar tissue from years of inflammation that can create a web between different surfaces of your TMJ. This web will prevent a lot of the movement you want to see in the joint. Only way to see the extent of this and cut out the web is through an arthroscopy. And the best way to prevent it/keep it from getting worse is through exercising and mobilization.

- It could also be from muscle tension. But truthfully this is less common than people will tell you. The fix is pretty simple; just slowly stretch, massage and heat over the course of 10-20min.
Headaches
Sometimes, headaches are just headaches. But if you deal with chronic headaches AND have TMJ Dysfunction, it’s more than likely that you’re dealing with muscle spasms/knots in the temporalis muscle.

The temporalis muscle is one of the two big muscles of mastication (chewing) that aids in closing your mouth. And as the name suggests, it connects up to your temples.
Since TMD patients often have problems with clenching or instability in their jaw system, it’s very common to develop tension in these big muscles along with little trigger points that can refer pain all over the head, neck, mouth, and jaw. You can deal with this pain as you would deal with any other muscle pain as we discussed previously in the “pain” part.
Ear Pain & Tinnitus
There is a very clear correlation between TMD and ear problems, such as pain, fullness, or tinnitus. The interesting part is that often nothing is necessarily wrong with the ear itself. TMD patients will go to an ENT and they won’t be able to help. It’s a TMJ issue. And here are some of the explanations I’ve found for it.
- The ligament connection
The TMJ and ear are incredibly close together, which is why you shouldn’t find it surprising that there is a physical link between them.
One of the strongest links is the “oto-mandibular” ligaments (literally ear-jaw ligaments). There are 2, but the biggest culprit connects between the retrodiscal tissue of the TMJ and a little bone in the ear called the “malleus” that plays an important role in transmitting the vibrations from sound to the inner ear.

This may sometimes be the culprit in feeling ear related symptoms because if you stretch this ligament you’re throwing the very sensitive ear system out of balance.
- The inflammatory connection
There’s a small bony gap located between the TMJ and the middle ear. It serves as a passageway for nerves and blood vessels as well as the disco malleolar ligament mentioned above. Because it’s a direct link between the TMJ and inner ear, it may become a pathway for inflammation to spread from the jaw joint to the ear.

It’s called the petrotympanic fissure, and when you deal with a bunch of inflammation in the TMJ, it can easily leak into middle ear structures and disturb the balances in pressure. Just keep in mind that this is a vast oversimplification.
- Eustachian Tube

This is a small passageway that runs between the middle ear and back of the throat as a sort of air pressure valve for the ear. It’s why your ears feel full when taking off in an airplane. This tube is normally “closed” to prevent infections from spreading to the ear and for keeping the air pressure stable. But when the outside air pressure changes rapidly, you feel it; until you yawn, chew, or swallow, which opens up the tube to equalize pressure again!
Unfortunately for us, this tube runs very close to the TMJ. Even the muscles used in opening and closing the tube are linked to jaw movement. If they can’t contract properly to open, you can get pressure build up in the ear.
Tightness and inflammation can also mess with the nerves needed to operate it.
- Nervous system

As mentioned, the trigeminal nerve has several branches that run near the TMJ. Importantly, the ones that control muscles responsible for controlling sound modulation in the ear.
It’s possible for these nerves to be compressed/entrapped by TMJ muscles or bones and cause tinnitus and pain. We can discuss further in the Trigeminal Neuralgia section below.
These ear problems can be pretty brutal because there’s not a lot of symptom relief out there. You have to work out the underlying problems with the TMJ or surrounding muscles. You can follow the postural and strengthening methods laid out in “the postural fix” section.
Trigeminal Neuralgia

The trigeminal nerve is the largest cranial nerve, responsible for facial sensation and jaw movement. It has three branches:
- Ophthalmic (V1) – Upper face & forehead
- Maxillary (V2) – Midface, cheeks, and upper teeth
- Mandibular (V3) – Jaw, lower teeth, and muscles for chewing
Because it connects to many areas, trigeminal nerve irritation can cause a wide range of symptoms, including facial numbness, headaches, sharp facial pain, tinnitus, ear issues, involuntary tear production, and salivary gland discomfort. This happens because the nerve influences salivary glands, tear glands, and muscles in the ear that help regulate sound.
Sometimes in cases of TMJ Dysfunction, these nerves can get entrapped and compressed, which may trigger chronic pain.
Two Common Trigeminal Nerve Entrapment Points in TMD:
- Auriculotemporal Nerve Entrapment (Costen’s Syndrome)

- This nerve (part of V3) runs behind the mandibular ramus near the TMJ.
- If the jaw is habitually retracted, the nerve can get compressed between the jawbone and the skull, causing pain, numbness, and ear-related symptoms.
- How to test it:
- Retract your jaw while opening/closing—if it triggers pain, this nerve is likely compressed.
- Press into the area manually to see if it reproduces symptoms.
- Buccal Nerve Entrapment (Within the Pterygoid Muscles)

- The buccal nerve (also part of V3) can get trapped between the lateral pterygoid muscles (which help move the jaw forward).
- This can create similar symptoms, since nerve compression spreads to nearby structures.
- How to test it:
- Try pushing your jaw forward against resistance—if this recreates your symptoms, the buccal nerve is likely trapped.
How to Fix It
- For Buccal Nerve Entrapment: Strengthen the lateral pterygoid muscle to keep the jaw properly positioned and free the nerve.
- For Costen’s syndrome you’ll want to work on protracting the jaw like we talked about in the postural section.
- Massaging the muscles may help temporarily decompress the nerves, but the real fix is strengthening the jaw and avoiding habitual retraction.
Forums, Support Groups, and Mindset
The TMJ Subreddit was my best friend when I first started dealing with TMD. Because the thing is that Google SUCKS these days. If you look up anything related to TMJ it feeds you the most generic and outdated information. At least on a forum you’ll have the real variety of experiences that exist in the TMJ world. Plus they’re great places to learn what to expect out of symptoms specific to you, or even upcoming surgeries you may have from people that have experienced it.
But unfortunately it comes with a LOT of noise. Think about how much bias, misinformation, and misunderstanding exists among doctors. Now imagine how much of that exists among random people typing online. It’s actually one of the biggest reasons I decided to write this - to cut out the noise. I know this ebook turned out long. But trust me, you’d spend 100x the amount of time figuring all this out through forums, research papers and doctors (like I did).
I will also warn you - there is a LOT of negativity and depression in these forums and support groups. I get it, I really do. It’s depressing to think about how bad things will get 10 years in the future, especially because TMDs develop at such an early age before other chronic disorders/ Why was I thinking about degenerative joint disease at 21 years old?
But some of these people just take it too far. It doesn’t help you to read other people’s negativity. And it doesn’t help you to get over your own. You don’t want to get stuck in an echochamber of depression. At the end of the day, we’ll all end up experiencing pain. It’s part of life. Do everything you can to treat it, but don’t let it ruin your happiness.
You can either be someone who catastrophizes the situation you’re in, or you can adapt to it. People who adapt have better results, so take that as you will.
I’m not a philosopher or life coach. You don’t have to take any of my advice. But I thought I’d put it in in case it resonates with someone with a similar experience.
At Home Manual Therapy Tutorials





X’s mark common trigger point locations, and the red marks where the pain can be felt. Some relief can be felt by looking for and targeting these spots with below exercises and other conservative treatment techniques.
Internal Masseter Release
Helps release tension and muscle pain from the masseter muscle.
- Use your thumb of your opposite hand to reach far back into your cheek.
- Gently bite to feel the muscle contract, and locate a tender spot.
- Gently pinch the muscle and hold the same pressure while your jaw muscles are relaxed.
- A typical hold is 60 seconds.
https://yourtmj.com/blogs/yourtmj-exercises/how-to-do-an-internal-masseter-release
Internal Masseter Mobilization
Helps release tension and muscle pain from the masseter muscle.
- Use your thumb of your opposite hand to reach far back into your cheek
- Gently bite to feel your muscle contract under your finger and relax
- Gently pinch the muscle from the highest position and pull down towards your chin
- You may also try to pull away from your ear and towards your cheek
- Repeat whichever technique you feel is most effective
https://yourtmj.com/blogs/yourtmj-exercises/how-to-do-the-internal-masseter-mobilization-for-tmj
Jaw Opening Mobilization
Helps release tension from muscles involved in clenching/closing your jaw. Also helps lightly mobilize the joint.
- Place your jaw in your hands so your pointer fingers are positioned just in front of your ears
- Compress your hands inward and gently pull them both down slightly.
- Let your jaw open as far as you feel comfortable and relax.
- You may have a partner help you open your jaw further by gently pulling down your chin.
- Make sure you move within a pain-free range of motion through the exercise.
https://yourtmj.com/blogs/yourtmj-exercises/how-to-do-a-jaw-opening-mobilization-for-tmj-jaw-pain
Lateral Jaw Glide
Helps mobilize both TMJs as well as working on strengthening lateral and medial pterygoids. Improves range of motion. Additionally works on neuromuscular connection to help ease jaw movement.
- Move your jaw to one side and hold briefly, then return to the starting position and repeat to the opposite side.
- Make sure to ease into the movement to avoid jaw pain.
- Try doing this exercise in front of a mirror to check the accuracy of your movements.
- Do 10 reps, once a day, 7 days a week.
https://yourtmj.com/blogs/yourtmj-exercises/how-to-do-a-lateral-jaw-glide-exercise-for-tmj-jaw-pain
Resisted Jaw Closing
Strengthens the upper head of the lateral pterygoid, masseter, temporalis, and medial pterygoid muscles. Also helps mobilize the TMJ and aims to improve range of motion.
- Open your mouth, and hold your chin with one hand so your thumb is on one side and your fingers are on the other side of your lower jaw.
- As you pull down with your hand, try to close your jaw.
- Once the jaw is closed, hold the bite for 3 seconds, then relax and repeat.
- Make sure you give a consistent amount of resistance with your hand throughout the exercise.
- Do not clench too hard, as that may exacerbate the condition.
Side-Lying Jaw Deviation Mobilization
Stretches and strengthens masseter, temporalis and medial pterygoid muscles. Slow mobilization of the joints, and helps improve range of motion and reduce stiffness.
- Begin lying on your side with your forehead supported.
- Relax your jaw so it hangs down. You may feel a slight stretch. Lift your jaw upward and pause briefly. Repeat.
- Make sure you move within a pain free range of motion throughout the exercise.
Controlled Jaw Opening with Tongue on Roof of Mouth
Helps improve neuromuscular connection, and improve symmetrical mouth opening. Works on isolating and training the lateral pterygoid for propoper opening. Isolates motion to only the “rotation” part of TMJ movement.
- Place your tongue on the roof of your mouth. Place each pointer finger on your TMJs, the bony bumps just inf front of your ears and under the cheekbone. Open and close your mouth slowly while keeping your tongue on the roof of your mouth, feeling in your fingers for symmetrical movement of the bones.
- One side may move more, so limit motion to the range in which both sides move equally. You may use a mirror to help guide your movement.
- Make sure to open only as far as is pain-free with your jaw remaining centered during the exercise.
One-sided forward jaw mobilization
Really small movement directly focused on the joint. Helps open up a little space which may help circulate joint lubrication and decompress the disc.
- Begin sitting upright. Place your thumb on top of your molars and lightly grip your jawbone. Place your other hand on the back of the jawbone.
- Gently press your jawbone down and back, then with your other hand gently press your jawbone forward. Hold, then relax and repeat for 10 reps.
- Make sure to keep your jaw relaxed and your movements gentle and slow. There should be little movement during the exercise.
Seated Jaw Distraction
Light decompression of the TMJ.
- Begin sitting upright with your jaw relaxed.
- Place your hands on the sides of your jawbone, and gently pull your jawbone down and back.
- Hold, then relax and repeat
- Make sure to keep your jaw relaxed and your movements gentle and slow. There should be little to no movement during the exercise.
- Do this exercise 7x Week; 1x Day; 1 Set; 10 Reps
External Jaw Release
Stretches the masseter and temporalis muscles.
- Place three fingertips just below each of your cheekbones so they are resting on the soft part of your jaw and in front of the jaw joint. Press your fingertips towards each other gently, as if you are squeezing a balloon, and pull gently towards the floor, allowing your jaw to softly open. Hold for at least 60 to 90 seconds, then relax and repeat for 10 reps.
- Try to release your jaw into the stretch and let your tongue hang out. Do not hold your jaw open. Instead, allow your jaw to release naturally as if you are falling asleep in a chair. Follow for more
- Do this exercise 7x Week; 1x Day; 2 Sets; 10 Reps
Seated One Sided Jaw Distraction
Similar to the forward jaw mobilization, except the movement is more focused on the decompression of the TMJ and opening that space up a little bit.
- Begin sitting upright.
- Place your thumb on top of your molars and lightly grip your jawbone. Gently press your jawbone down and back. Hold, then relax and repeat.
- Make sure to keep your jaw relaxed and your movements gentle and slow. There should be little movement during the exercise.
Do this exercise 7x Week; 1x Day; 1 Sets; 10 Reps
Isometric Jaw Abduction
Strengthens lateral pterygoids
- Begin sitting upright.
- Place your fist under your chin and apply a gentle pressure as you try to open your jaw slightly. Hold for 3 seconds, and repeat for 2 sets of 10.
- Make sure not to let your jaw shift to either side during the exercise.
Isometric Jaw Deviation
Strengthens lateral and medial pterygoids.
- Begin sitting in an upright position.
- Place your hand on one side of your jaw and let your mouth open slightly. Apply a gentle pressure as you try to move your jaw sideways against your hand. Hold for 3 seconds. Relax, then repeat for 2 sets of 10.
- There should be little to no movement during the exercise. Share with someone that needs it.
Lateral and Medial Glide Mobilization
Stretches/decompresses the TMJ. So keep it light and slow.
- Place one hand on the same side between your ear and cheek. While keeping your jaw relaxed, apply gentle pressure to your upper jaw for a light stretch on either joint. Make sure to keep your neck stable. Do not allow your head to tilt.
- Make sure you move within a pain-free range of motion throughout the exercise. Tag someone who needs it.
Internal Lateral Pterygoid Release
Pretty much the only way to release tension/spasms from the lateral pterygoid. Great for if your clicking is flaring up, or just as another place to check for muscle pain.
- Open your mouth and use your opposite hand’s pinky to trace your top teeth all the way back
- Follow bone as high up and back as you can go
- Close your mouth slightly whale maintaining a tolerable amount of pressure ot this region as your jaw muscles relax
- Make sure your fingernail is cut short to protect your gums, and remember this is a very sensitive area; especially for people with TMJ Disorders.
External Medial Pterygoid Release
The medial pterygoid is a tough muscle to reach. Here you can try to release it from its attachment point at the lower jaw bone. It’s a place to check for where muscle pain could be coming from.
- Trace your thumb to the back of your lower jawbone, right at the rounding that transitions from the horizontal to the vertical part of the bone
- Let your jaw muscles relax, and press your thumb under this area between your jawbone and neck. You’re pressing into where the muscle connects to your jaw.
- Make sure to avoid the lymph node that sits just in front of this spot (it’ll be a noticeable bump). There are also salivary glands, so if you start to salivate, that may be the sore spot.
- You’ll have an easier time getting into it if you tuck your chin down.
Internal Medial Pterygoid Release
Another way to check for where muscle pain can be coming from. You can release tension/spasm from the medial pterygoid form indie the mouth.
- Slide your index finger down inside of your cheek. The pad side is against the cheek, and the nail side up against the molars.
- When you get to the back of the molars you will bump into bone.
- Open your jaw and slide your finger in to the inner side of that bone.
- The medial pterygoid is right there, apply mild to moderate pressure and wait for it to relax.
- WARNING: You may activate your gag reflex doing this. Take it slow.
Rocabado's 6x6 Exercise Routine
Rocabado 6x6 exercises are well-known physical therapy routines for TMJ pain relief, involving a series of jaw exercises:
- Rest Position of the Tongue: Place the tip of your tongue on the roof of your mouth, applying gentle pressure.
- Control of TMJ Rotation: Open and close your jaw while gently pressing the tip of your tongue on the palate.
- Rhythmic Stabilization Technique: Place two fingers on your chin. Open and close your jaw while pressing your tongue on the palate.
- Axial Extension of the Neck: Lift and lower your chin as if nodding.
- Shoulder Posture: Squeeze your shoulder blades together while lifting and lowering your chest.
- Stabilized Head Flexion: Bring your chin towards your neck (creating a "double chin"), then push it out again.
Kraus' TMJ Exercises
Physical therapist Steve Kraus developed these exercises to limit the activity of the chewing muscles:
- Tongue Position at Rest: Place the tip of your tongue on the roof of your mouth, just behind your front teeth.
- Teeth Apart: Keep your upper and lower teeth apart to help relax your jaw.
- Nasal-Diaphragmatic Breathing: Breathe through your nose to better position your teeth and tongue.
- Tongue Up and Wiggle: Place your tongue on the palate, then move your jaw side to side.
- Strengthening: Place a stack of tongue depressors between your upper and lower teeth. Use enough depressors to give your jaw a good stretch. Hold for up to five minutes a few times a day.
- Tooth and Bite: Place an index finger on an upper canine tooth and try to bite it. Repeat five to 10 times, up to eight times a day.
Intro to At Home Myofunctional Therapy
As we discussed in the root cause and postural section of the book, there’s a connection between the strength of your tongue, palettal, facial muscles and your TMJ wellness. It may be helpful to try these exercises for a few weeks to see if they help - especially if you also have problems with sleep and breathing.
https://www.sleepclinic.be/wp-content/uploads/Myofunctional-Therapy-to-Improve-Sleep-Apnea-.pdf
Product Recommendations:
yourTMJ Pen:

Ok, to be fair, there’s a lot of bias with this product because I’m the one who designed it. But as of now, it’s still the only TMJ massager that ACTUALLY heats up while simultaneously letting you dig into jaw muscle tissue AND vibrating to mask some of the pain that comes from trigger point release.
You have no idea how many cheap amazon “TMJ massagers” (they’re just repackaged skin care tools or lactation massagers) I’ve bought and had to return because they didn’t heat more than 100F. For heat to even work as an analgesic (pain blocker) it needs to be at least 104F according to research, and for short periods of time closer to 114F.
Also, none actually help you MASSAGE the TMJ muscles. They just feel good on the skin, whereas what you need is to apply deep pressure into the muscles to dig into and release those trigger points.
That’s why I ended up building yourTMJ Pen. As I’ve explained, heated massage isn’t a root cause treatment/cure. It’s a day to day muscle pain/tension management tool. Heated massage worked for me, so I needed it to be more convenient.
Here’s a link if you’re interested, and you can use code WELCOME25 for a discount.
ClenchRelief:

Splints can be really expensive, which is why I think this is such a genius product. You’ll find a lot of “boil and bite” nightguards out there… these do NOTHING for TMD. As we’ve discussed, the point of a splint is to at least temporarily reposition your lower jaw to decompress the TMJ.
This one by ClenchRelief uses this little plastic piece to hold your jaw slightly forward (those 2-4mm we discussed) while a putty sets and molds itself around the teeth. Then you remove the plastic piece and boom, you instantly have a custom fit splint for under $150 delivered to your door.
One warning though is that it only has tooth coverage on the molars. So I wouldn’t recommend wearing it at all times in the day for a long period of time, but for just nighttime use, or just to put it on here and there for some relief is totally fine.
Really smart solution: And I managed to snag 10% off for you guys here
REMplenish Water Bottle:

If you have trouble keeping your tongue at the roof of your mouth, breathing through your nose, and something like snoring - it may be a sign to look into myofunctional therapy. We listed a bunch of exercises you can do, but this product is actually pretty genius and may make things a lot easier.
Basically, it’s a water bottle with a straw designed to help your tongue and mouth muscles strengthen while you drink. I looked into it and the research behind it is really strong.
https://www.remasteredsleep.com/NOAM83365
Still not out but I’m on the lookout:
Understanding whether your clench in your sleep is extremely important as we’ve learned. And tracking something is the best start to figuring out what helps reduce it. Like maybe sleeping on your side eliminates it. Maybe postural exercises reduce it over time. Maybe a certain supplement helps. Maybe a splint makes things better, or maybe it makes things worse.
That’s why I think a technology that will give you a noninvasive method to measure clenching activity at night will be a game changer. Currently, there aren’t any that are good enough. But I found these guys that are working on exactly what I imagined and talked to the founder (he’s legit): https://www.jawsense.com/
Sources:
Landmark National Academy of Medicine Report (Overview):
https://tmj.org/hope-in-research/landmark-studies/national-academy-of-medicine/
Landmark Orofacial Pain: Prospective Evaluation and Risk Assessment (OPPERA) Study (Overview)
https://tmj.org/hope-in-research/landmark-studies/oppera-study/
Jaw muscles are measurably overactive when the jaw is imbalanced:
https://deepblue.lib.umich.edu/bitstream/handle/2027.42/25483/0000023.pdf?sequence=1
Deep dive into the anatomy and movement of the TMJ
https://clinicalgate.com/kinesiology-of-mastication-and-ventilation/
Treatment of TMJD from the Dental Perspective
https://pocketdentistry.com/13-treatment-of-temporomandibular-joint-disorders/
Idiopathic Condylar Resorption from Orthodontic Perspectivehttps://pocketdentistry.com/idiopathicprogressive-condylar-resorption-an-orthodontic-perspective/
Clinical Analysis of the postural fix for TMJD
https://mskneurology.com/true-cause-solution-temporomandibular-dysfunction-tmd/
“Significant correlation between poor posture and the occurrence of TMD”
https://pmc.ncbi.nlm.nih.gov/articles/PMC10095000/
Why movement is SO important for TMJ
https://pubmed.ncbi.nlm.nih.gov/2579224/
When a TMJ on one side is damaged, the other side has to compensate
https://link.springer.com/article/10.1007/s10439-023-03424-6?
“Manual therapy significantly improved pain and mouth opening compared to baseline”
https://pmc.ncbi.nlm.nih.gov/articles/PMC7690916/
Heat Treatment for TMJ Disorders: “Shown to relieve pain, reduce muscle tension, improve manudibular function, and increase mouth opening”
https://doi.org/10.1590/2317-1782/20152014148
https://www.scielo.br/j/codas/a/ZQ4BNzY3Ztv3KFWNNB6TtVc/?lang=en
Analgesic (Pain Killing) Effects of Heat
https://pmc.ncbi.nlm.nih.gov/articles/PMC7434528/
Difference between dry and moist heat is negligible - so use whichever you prefer
In depth review of arthrocentesis and its benefits/risks
https://pmc.ncbi.nlm.nih.gov/articles/PMC6585213/
Success rates of TMJ Arthroscopy
https://pubmed.ncbi.nlm.nih.gov/11467389/
TMJA Overview of Splint Therapy
https://tmj.org/living-with-tmj/treatments/splints/
The TMJ Retrodiscal tissue CAN remodel! Goat study
https://pubmed.ncbi.nlm.nih.gov/10561723/
TMJ Closed Lock often improves on its own
Internal derangements of the TMJ (Textbook chapter for Maxillofacial surgeons)
https://link.springer.com/chapter/10.1007/978-981-15-1346-6_63




2 comments
Very informative article explaining TMJ symptoms and treatment options clearly. Helpful insights for understanding jaw pain and improving daily comfort.
Informative guide explaining TMJ causes, symptoms, and treatment options clearly. Helpful resource for anyone seeking jaw pain relief.